
Are GLP-1s Bending the Obesity Curve?
ABSTRACT
For six consecutive decades, adult obesity prevalence in the United States followed an unbroken upward trajectory, rising from approximately 13% in 1960 to nearly 42% by 2020 (NHANES/CDC). In 2022, the Gallup National Health and Well-Being Index recorded a peak adult obesity rate of 39.9%. By 2025, that figure had declined to 37.0%, representing approximately 7.6 million fewer obese American adults. This decline coincides temporally with an unprecedented surge in GLP-1 receptor agonist (GLP-1 RA) adoption, which has grown from 1.5 million active users in 2021 to an estimated 15 million in 2026. This guide evaluates the hypothesis that GLP-1 receptor agonist adoption is contributing to a meaningful inflection in the U.S. obesity curve. We examine NHANES historical trends, Gallup and BRFSS surveillance data, the temporal correlation between GLP-1 prescription growth and obesity rate decline, and alternative contributing factors including the disproportionate impact of COVID-19 on obese Americans (78% of hospitalizations involved overweight or obese individuals) as a catalyst for health consciousness, and the broader cultural shift toward health awareness captured in the "Health is Wealth" movement. We present a multi-factorial framework that considers GLP-1 pharmacotherapy, pandemic-driven mortality awareness, and cultural health consciousness as convergent forces that may be collectively bending the obesity curve for the first time in modern American history.
TABLE OF CONTENTS
- 1. Introduction: Six Decades of Unbroken Ascent
- 2. NHANES Historical Trends: The Epidemiological Record (1960-2023)
- 3. The GLP-1 Surge: Adoption, Scale, and Demographic Patterns
- 4. Temporal Correlation: GLP-1 Adoption and Obesity Decline
- 5. COVID-19 as a Catalyst: When a Pandemic Exposed the Obesity Crisis
- 6. The Health Awareness Revolution: "Health Is Wealth"
- 7. A Multi-Factorial Framework: Three Convergent Forces
- 8. Limitations and Confounders
- 9. Clinical Implications
- 10. Conclusion
- References
- About the Author
- Intellectual Property and Disclosure
1. Introduction: Six Decades of Unbroken Ascent
The prevalence of obesity among American adults has followed a remarkably consistent upward trajectory for more than sixty years. Data from the National Health and Nutrition Examination Survey (NHANES), administered by the CDC's National Center for Health Statistics (NCHS), provide the most rigorous longitudinal record of this trend, based on measured (not selfreported) height and weight data from nationally representative samples.
The historical record is striking in its monotonic progression:
- 1960-1962 (NHES I): Adult obesity prevalence approximately 13.4%
- 1971-1974 (NHANES I): 14.5%
- 1976-1980 (NHANES II): 15.0%
- 1988-1994 (NHANES III): 22.9%, marking the beginning of accelerated growth
- 1999-2000: 30.5%, crossing the 30% threshold for the first time
- 2007-2008: 33.7%
- 2015-2016: 39.6%
- 2017-2018: 42.4%, the highest measured NHANES prevalence
- 2021-2023 (most recent NHANES data): 40.3%
For six decades, no public health intervention, dietary guideline revision, exercise campaign, or policy initiative produced a meaningful, sustained reversal in this trend. The obesity rate rose through every presidential administration, every dietary era (low-fat, low-carb, Mediterranean), every fitness movement, and every public health campaign. The curve appeared unbreakable.
Source: CDC/NCHS, National Health and Nutrition Examination Survey (NHANES), 1960-2023.
Emmerich SD, Fryar CD, Stierman B, Ogden CL. Obesity and Severe Obesity Prevalence in Adults: United States, August 2021-August 2023. NCHS Data Brief No. 508, September 2024.
Then, beginning in 2022-2023, something changed. Multiple independent surveillance systems began detecting a slowdown, plateau, or outright decline in adult obesity prevalence. This guide evaluates the evidence for this inflection and examines the forces that may be driving it.
2. NHANES Historical Trends: The Epidemiological Record (1960-2023)
The NHANES dataset represents the gold standard for obesity surveillance in the United States. Unlike self-reported surveys, NHANES uses standardized physical examinations with measured height and weight, eliminating the "vanity bias" that typically causes self-reported data to underestimate obesity prevalence by 3 to 5 percentage points.
2.1 The Acceleration Phase (1988-2018)
The most dramatic period of obesity growth occurred between 1988 and 2018, when prevalence nearly doubled from 22.9% to 42.4%. Several factors drove this acceleration:
- The proliferation of ultra-processed foods: by 2018, ultra-processed foods constituted approximately 58% of total caloric intake for American adults
- Increasing sedentary behavior: screen time, desk-based employment, and automobiledependent infrastructure reduced daily physical activity
- Portion size inflation: restaurant and packaged food portions increased by 2 to 3-fold between 1970 and 2010
- Socioeconomic disparities: food deserts, limited access to healthcare, and structural barriers to physical activity disproportionately affected low-income and minority communities
- Sleep disruption: average sleep duration for American adults declined from 7.9 hours in 1960 to 6.8 hours by 2018, with chronic sleep deprivation independently promoting weight gain through hormonal dysregulation
2.2 The Potential Inflection (2020-2023)
The most recent NHANES cycle (August 2021-August 2023) reported an age-adjusted adult obesity prevalence of 40.3%. While still alarmingly high, this represents a potentially significant data point: the first NHANES cycle in which obesity prevalence did not increase significantly compared to the prior decade. The NCHS Data Brief No. 508 (September 2024) noted that "from 2013-2014 through August 2021-August 2023, the age-adjusted prevalence of obesity did not change significantly."
This plateau in the most rigorous dataset available stands in contrast to the continuously rising trajectory of the prior three decades. Whether this represents a true inflection or a temporary pause requires ongoing surveillance, but it is epidemiologically noteworthy.
3. The GLP-1 Surge: Adoption, Scale, and Demographic Patterns
The rise of GLP-1 receptor agonist therapy represents one of the most rapid pharmaceutical adoption events in modern medical history. Understanding the scale and demographics of this adoption is essential for evaluating its potential population-level impact on obesity prevalence.
© 2026 Dr. Haad Mahmood, MD. All rights reserved. Original intellectual property. Reproduction prohibited without written permission.
Mahmood H. GLP-1 Adoption in America: A 5-Year Surge. HaadMD. 2026. https://haadmd.com. Data: J.P. Morgan Research (2026), IQVIA, KFF Health Tracking Poll (2025), Gallup, FAIR Health, RAND Corporation.
3.1 The Scale of Adoption
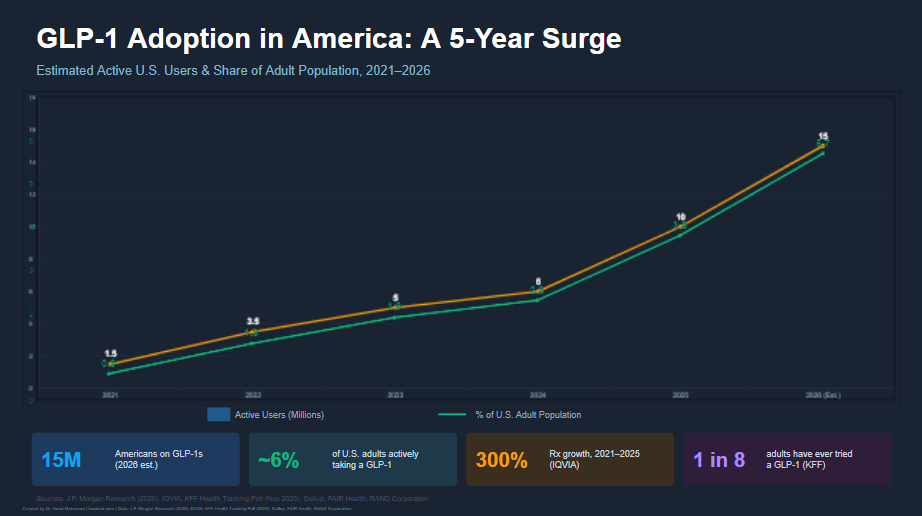
The growth trajectory of GLP-1 receptor agonist prescriptions has been extraordinary:
- 2021: Approximately 1.5 million active users (0.6% of U.S. adult population). Wegovy (semaglutide 2.4 mg for weight management) received FDA approval in June 2021
- 2022: 3.5 million active users (1.3%). Clinical trial results from STEP and SURMOUNT programs generated significant media coverage and public awareness
- 2023: 5 million active users (1.9%). Supply shortages reflected demand outstripping manufacturing capacity
- 2024: 6 million active users (2.3%). Tirzepatide (Zepbound) received FDA approval for weight management, expanding the market
- 2025: 10 million active users (3.8%). GLP-1 use more than doubled, with 12.4% of adults reporting having ever used an injectable for weight loss (Gallup, 2025)
- 2026 (estimated): 15 million active users (~5.7% of adult population). 1 in 8 American adults have tried a GLP-1 receptor agonist (KFF, November 2025)
3.2 Demographic Patterns of Adoption
GLP-1 adoption has not been uniform across demographics. Data from the Gallup National Health and Well-Being Index reveal important patterns:
- Women have adopted GLP-1 therapy at significantly higher rates than men: 15.2% vs. 9.7% ever-use as of 2025
- Age groups 40 to 49 (16.2% usage) and 50 to 64 (17.0% usage) show the highest adoption rates
- Younger adults (18 to 29) show the lowest adoption rates despite increasing obesity prevalence in this demographic
- Seniors (65+) report 11.1% usage but report less weight loss benefit compared to younger groups
4. Temporal Correlation: GLP-1 Adoption and Obesity Decline
The temporal alignment between GLP-1 adoption and obesity decline is the most provocative element of this epidemiological analysis. Multiple independent data sources now show convergent trends.
© 2026 Dr. Haad Mahmood, MD. All rights reserved. Original intellectual property. Reproduction prohibited without written permission.
Mahmood H. Are GLP-1s Bending the Obesity Curve? HaadMD. 2026. https://haadmd.com. Data: Gallup National Health and WellBeing Index (2025).
4.1 The Gallup Data: A 2.9 Percentage Point Decline
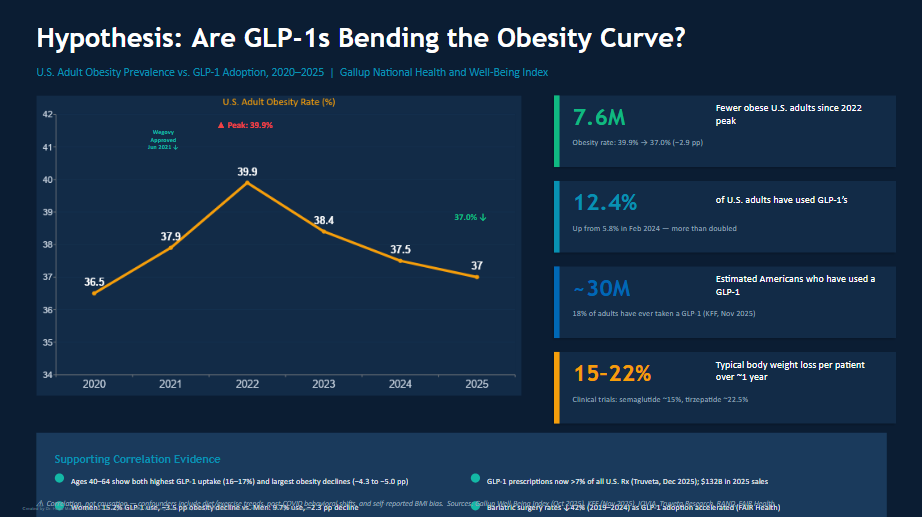
The Gallup National Health and Well-Being Index, based on surveys of 16,946 U.S. adults across three nationally representative samples in 2025, documents the following obesity prevalence trajectory:
- 2022: 39.9% (peak)
- 2023: 38.4% (initial decline)
- 2024: 37.5% (continued decline)
- 2025: 37.0% (lowest in three years)
This 2.9 percentage-point decline over three years represents approximately 7.6 million fewer obese American adults. While the Gallup methodology uses self-reported height and weight (subject to vanity bias), Gallup notes that its methods have been consistent over time, making the trend directionally reliable even if absolute values are slightly underestimated.
4.2 Corroborating Data Sources
The Gallup findings are supported by independent data sources:
- BRFSS (Behavioral Risk Factor Surveillance System) 2024: The Trust for America's Health (TFAH) 2025 State of Obesity Report found that the number of states with adult obesity rates at or above 35% decreased from 23 to 19, the first-ever decline in this metric
- JAMA Health Forum (December 2024): Rader et al. analyzed 16.7 million BMI measurements from 2013 to 2023 (Optum data) and identified a deceleration and potential reversal in the obesity trend beginning in 2022-2023
- NHANES 2021-2023: As noted in Section 2, the first NHANES cycle in 30 years without significant obesity increase
4.3 Correlation vs. Causation
The temporal correlation between GLP-1 adoption and obesity decline is strong but does not establish causation. Several factors complicate a direct causal attribution:
- The 2.9 percentage-point decline in the Gallup data translates to roughly 7.6 million fewer obese adults. Current GLP-1 active users number approximately 10 to 15 million, with average weight loss of 15 to 22% of body weight, suggesting plausible but not exclusive pharmacologic contribution
- GLP-1 medications produce 15 to 22% mean body weight loss in clinical trials, sufficient to move many users from obese (BMI 30+) to overweight (BMI 25 to 29.9) status
- The strongest obesity declines are in demographic groups with the highest GLP-1 usage (ages 40 to 64, women), supporting a dose-response relationship at the population level
- However, the decline began in 2022-2023, when GLP-1 adoption was still relatively limited (3.5 to 5 million users), suggesting other contributing factors
5. COVID-19 as a Catalyst: When a Pandemic Exposed the Obesity Crisis
The COVID-19 pandemic, which killed approximately 1.2 million Americans between 2020 and 2024, served as an unprecedented catalyst for obesity awareness. The virus did not affect all populations equally, and its disproportionate impact on obese and overweight individuals was widely publicized and deeply felt.
5.1 The Disproportionate Toll on Obese Americans
The CDC published data demonstrating the stark relationship between body weight and COVID19 outcomes:
- 78% of Americans hospitalized for COVID-19 were overweight or obese (CDC, March 2021). Of those hospitalized, 27.8% were overweight and 50.2% were obese
- The risk of hospitalization, ICU admission, and death increased sharply with rising BMI, particularly among individuals aged 65 and older
- Obesity was identified as an independent risk factor for COVID-19 mortality, even after controlling for age, sex, race, and other comorbidities
- Individuals with severe obesity (BMI 40+) had the highest risk of ventilator requirement and death
- The relationship between obesity and COVID-19 severity was widely reported in mainstream media, social media, and public health communications, creating a population-level awareness event unlike any in the history of the obesity epidemic
5.2 The "Survivorship Selection" Hypothesis
A darker but epidemiologically relevant consideration is survivorship selection. COVID-19 disproportionately killed obese Americans:
- An estimated 1.2 million Americans died from COVID-19, with overweight and obesity present in approximately 78% of fatal cases
- This mortality was concentrated in older and more severely obese populations
- The selective mortality of obese individuals may have directly contributed to a modest mathematical decrease in obesity prevalence by removing individuals with the highest BMIs from the living population
- While this effect alone cannot account for the observed 2.9 percentage-point decline (the absolute number of COVID deaths, while tragic, is small relative to the 130+ million obese adults in the U.S.), it represents a measurable contributing factor
This is not a desirable mechanism for obesity reduction. It is, however, an epidemiologically relevant factor that must be acknowledged when evaluating population-level obesity trends during the 2020-2025 period.
5.3 COVID-19 as an Awareness Accelerant
Perhaps more impactful than survivorship selection was the awareness effect. The pandemic made the consequences of obesity visceral, personal, and immediate in ways that decades of public health messaging had failed to achieve:
- Millions of Americans personally knew someone who was hospitalized or died from COVID-19, and witnessed the role that obesity played in severe outcomes
- Media coverage of the obesity-COVID connection reached virtually every American household, creating a level of public health awareness that no government campaign had achieved
- The pandemic forced a national conversation about metabolic health, immune function, and the personal responsibility of maintaining a healthy body weight
- For the first time, obesity was widely framed not just as a chronic disease risk factor but as an acute survival threat in the context of infectious disease
- This awareness created a receptive population primed for GLP-1 adoption when these medications became widely available in 2022-2024
6. The Health Awareness Revolution: "Health Is Wealth"
The period from 2020 to 2026 has witnessed a profound cultural shift in how Americans relate to their health. This movement, often captured in the phrase "Health is Wealth," represents a convergence of pandemic trauma, social media health content, wearable technology adoption, and a generational reorientation toward wellness as a core personal value.
6.1 The Post-Pandemic Wellness Boom
COVID-19 did not merely create fear; it created motivation. In the aftermath of the pandemic:
- Gym membership and fitness app subscriptions surged to all-time highs by 2023-2024, rebounding far beyond pre-pandemic levels
- The global wellness economy grew to an estimated $6.3 trillion by 2025, with the U.S. representing the largest single market
- Wearable health technology (Apple Watch, Oura Ring, Whoop, continuous glucose monitors) achieved mainstream adoption, making health metrics visible and gamified for millions of consumers
- Social media platforms became dominant channels for health and fitness content, with health-focused influencers reaching audiences of tens of millions
- Functional medicine, integrative health, and "biohacking" moved from niche to mainstream, with consumers actively seeking metabolic optimization beyond traditional disease management
6.2 Generational Health Consciousness
The health awareness shift is particularly pronounced in younger demographics:
- Gen Z and Millennials report significantly higher health consciousness than prior generations at equivalent ages
- Alcohol consumption has declined among younger adults, with "sober curious" and mindful drinking movements gaining cultural traction
- Plant-forward and whole-food diets have gained significant market share, with ultraprocessed food consumption beginning to show signs of plateauing
- Mental health awareness has destigmatized stress management, sleep optimization, and holistic wellness approaches
6.3 "Health Is Wealth" as a Cultural Paradigm
The phrase "Health is Wealth" has evolved from a proverb to a cultural movement. It reflects a fundamental reorientation of values:
- Financial wellness and physical wellness are increasingly seen as inseparable. Employers now invest in employee health programs as retention and productivity tools
- Preventive health spending has increased as consumers shift from reactive healthcare (treating disease after it develops) to proactive health optimization
- The democratization of health information through podcasts, social media, and directto-consumer lab testing has empowered individuals to take ownership of their metabolic health
- Celebrity and public figure transparency about GLP-1 use has reduced stigma and normalized pharmacologic weight management as a legitimate health tool rather than a sign of failure
7. A Multi-Factorial Framework: Three Convergent Forces
The evidence suggests that the observed inflection in the U.S. obesity curve is not attributable to any single factor but rather to the unprecedented convergence of three forces that are simultaneously and synergistically acting on population-level obesity prevalence.
7.1 Force 1: GLP-1 Pharmacotherapy at Scale
- 15 million active users by 2026 (approximately 6% of U.S. adults)
- Clinical efficacy of 15 to 22% mean body weight loss
- Demographic-specific dose-response correlation between usage rates and obesity decline
- Continued market expansion with new agents (retatrutide, orforglipron, oral semaglutide) and improved insurance coverage
7.2 Force 2: COVID-19 Mortality and Awareness
- 1.2 million American deaths with 78% of hospitalizations involving overweight or obese individuals
- Modest survivorship selection effect reducing absolute number of obese individuals in the population
- Profound awareness effect transforming obesity from abstract chronic risk to immediate survival concern
- Creation of a psychologically receptive population primed for GLP-1 adoption and health behavior change
7.3 Force 3: The "Health Is Wealth" Cultural Shift
- Post-pandemic wellness boom with record gym memberships, fitness app adoption, and wearable technology penetration
- Generational reorientation toward health consciousness, particularly among Gen Z and Millennials
- Democratization of health information and metabolic literacy through social media and podcasts
- Destigmatization of pharmacologic weight management, enabling broader GLP-1 adoption without shame
These three forces are not merely additive; they are synergistic. COVID-19 created the awareness and urgency. The "Health is Wealth" movement created the cultural receptivity. And GLP-1 pharmacotherapy provided the most effective tool ever available for weight management at scale. None of these forces alone would likely have produced the observed inflection. Together, they represent a genuinely novel epidemiological moment.
8. Limitations and Confounders
Any epidemiological evaluation of this hypothesis must acknowledge significant limitations:
- Ecological fallacy: population-level correlations (GLP-1 adoption vs. obesity decline) do not prove individual-level causation. Individuals using GLP-1s may not be the same individuals contributing to the observed obesity decline in survey data
- Self-reported data limitations: Gallup and BRFSS data rely on self-reported height and weight, which systematically underestimates obesity prevalence. Trends are directionally reliable, but absolute values carry known bias
- Temporal lag: the obesity decline began in 2022-2023 when GLP-1 adoption was still modest (3 to 5 million users), suggesting that GLP-1 pharmacotherapy alone cannot fully explain the initial inflection
- Discontinuation effects: GLP-1 medications are associated with significant weight regain upon discontinuation (approximately two-thirds of weight lost is regained within one year of stopping therapy). The durability of the population-level effect depends on sustained adherence, which remains uncertain
- Insurance and access barriers: GLP-1 medications remain expensive ($800 to $1,500+ per month without insurance), and coverage varies significantly. The populations most affected by obesity (lower-income, racial/ethnic minorities) may have the least access to these medications
- Competing explanations: economic factors, changes in food industry practices, evolving dietary patterns, and other unmeasured confounders may contribute to the observed trend
- COVID-19 survivorship effect: the magnitude of the survivorship selection effect is difficult to quantify precisely, and it is not a replicable or desirable public health mechanism
9. Clinical Implications
- Recognize that population-level obesity reduction is now measurable and real. For the first time in six decades, multiple independent data sources show obesity prevalence declining or plateauing. Clinicians should be aware that the epidemiological environment is changing.
- GLP-1 receptor agonist therapy should be considered as a population health intervention, not merely individual pharmacotherapy. At 15 million active users, GLP-1s are now operating at a scale where individual treatment outcomes aggregate into populationlevel epidemiological signal.
- Leverage the "Health is Wealth" cultural moment. Patient readiness for health behavior change is at an all-time high. Clinicians should capitalize on this by integrating lifestyle modification counseling with pharmacologic therapy, recognizing that cultural receptivity amplifies treatment effectiveness.
- Address the COVID-19 awareness legacy. Many patients now understand that obesity is not merely a cosmetic concern or chronic disease risk factor but a survival risk. This awareness can be leveraged for patient motivation and engagement.
- Advocate for equitable GLP-1 access. The populations most burdened by obesity often have the least access to GLP-1 therapy. Clinicians should advocate for insurance coverage expansion, patient assistance programs, and compounding pharmacy access to ensure that pharmacologic weight management reaches all populations.
- Monitor for sustainability. The durability of the obesity curve inflection depends on sustained GLP-1 adherence, continued cultural health awareness, and policy support. Clinicians should counsel patients on long-term weight management strategies beyond pharmacotherapy alone.
- Integrate the 80/20 Framework. As described in the companion publication, medication accounts for approximately 20% of therapeutic success. The remaining 80% depends on patientdriven lifestyle modifications. The convergence of pharmacology and cultural readiness makes this the ideal moment to implement the 80/20 approach.
10. Conclusion
For sixty years, the U.S. obesity curve moved in only one direction: up. No dietary guideline, exercise campaign, public health initiative, or pharmacologic intervention produced a sustained population-level reversal. The curve appeared immovable.
The period from 2022 to 2025 may represent the first genuine inflection point in this trajectory. The Gallup National Health and Well-Being Index records a 2.9 percentage-point decline in adult obesity prevalence (39.9% to 37.0%), representing 7.6 million fewer obese Americans. BRFSS data show the first-ever decline in the number of states with obesity rates above 35%. NHANES shows its first cycle in 30 years without significant obesity increase. And a December 2024 analysis of 16.7 million BMI measurements in JAMA Health Forum identified a deceleration and potential reversal in the obesity trend.
The hypothesis that GLP-1 receptor agonists are bending the obesity curve is supported by the temporal correlation, the demographic dose-response pattern, and the clinical efficacy data. However, the evidence suggests that GLP-1 pharmacotherapy is one component of a multifactorial inflection driven by three convergent forces: GLP-1 adoption at unprecedented scale, the awareness legacy of COVID-19 (which killed 1.2 million Americans and exposed obesity as an acute survival threat), and the "Health is Wealth" cultural revolution that has transformed how Americans relate to their bodies, their health, and their personal responsibility for metabolic wellness.
These three forces are synergistic. COVID-19 created the urgency. Cultural health consciousness created the receptivity. And GLP-1 pharmacotherapy provided the tool. Whether this inflection is sustained will depend on continued GLP-1 access and adherence, durable cultural health awareness, and policy commitment to addressing the structural determinants of obesity.
The obesity curve may be bending. The task now is to ensure it keeps bending.
The curve didn't bend because of a virus.
The curve didn't bend because of a cultural moment.
It bent because all three happened at once."
~ Dr. Haad Mahmood, MD
References
- CDC/NCHS. National Health and Nutrition Examination Survey (NHANES). Obesity Prevalence in U.S. Adults, 1960-2023. Hyattsville, MD: National Center for Health Statistics.
- Emmerich SD, Fryar CD, Stierman B, Ogden CL. Obesity and Severe Obesity Prevalence in Adults: United States, August 2021-August 2023. NCHS Data Brief No. 508. September 2024.
- Gallup National Health and Well-Being Index. U.S. Adult Obesity Rate, 2020-2025. Based on surveys of 16,946 U.S. adults, 2025.
- Rader B, Hazan R, Brownstein JS. Changes in Adult Obesity Trends in the US. JAMA Health Forum. 2024;5(12):e243685.
- Trust for America's Health (TFAH). State of Obesity Report 2025: Better Policies for a Healthier America. October 2025. Analysis of 2024 BRFSS data.
- CDC COVID-19 Response Team. Body Mass Index and Risk for COVID-19-Related Hospitalization, Intensive Care Unit Admission, Invasive Mechanical Ventilation, and Death. MMWR. 2021;70(10):355-361.
- Kompaniyets L, Goodman AB, Belay B, et al. Body Mass Index and Risk for COVID-19-Related Hospitalization, Intensive Care Unit Admission, Invasive Mechanical Ventilation, and Death. CDC MMWR. March 2021.
- J.P. Morgan Research. GLP-1 Market Landscape and Adoption Projections. January 2026.
- IQVIA National Prescription Audit. GLP-1 Receptor Agonist Prescription Volumes, 2021-2025.
- KFF Health Tracking Poll. November 2025. GLP-1 Usage and Weight Loss Medication Trends.
- Gallup/West Health Healthcare Survey. GLP-1 Injectable Weight Loss Medication Usage by Demographics, 2024-2025.
- NCHS. Provisional COVID-19 Mortality Surveillance. National Vital Statistics System (NVSS). Total U.S. COVID19 deaths, 2020-2024.
- Silva-Lalucci MP, et al. Obesity as a Risk Factor for Complications and Mortality in Individuals with SARS-CoV-2: A Systematic Review. Nutrients. 2024;16(4):543.
- Mahmood H. GLP-1 Adoption in America: A 5-Year Surge [Figure 1]. Correlating GLP-1 Outcomes with Advanced Lab Panels: Cytokines, Metabolic Markers, and Hormones. 2026. Original intellectual property of Dr. Haad Mahmood, MD.
- Mahmood H. Are GLP-1s Bending the Obesity Curve? [Figure 2]. Correlating GLP-1 Outcomes with Advanced Lab Panels: Cytokines, Metabolic Markers, and Hormones. 2026. Original intellectual property of Dr. Haad Mahmood, MD.
- Mahmood H. The Physician's Definitive Guide to Maximizing GLP-1 Outcomes: The 80/20 Framework. HaadMD Clinical Reference Series. April 2026.
- Global Wellness Institute. Global Wellness Economy Monitor. 2025 Estimates.