
The Physician’s Definitive Guide to Maximizing GLP-1 Outcomes
ABSTRACT
GLP-1 receptor agonist (GLP-1 RA) therapies have demonstrated significant efficacy in weight management, with clinical trials reporting 15–22% mean body weight reduction. However, clinical response remains highly heterogeneous, ranging from <5% to >20% weight loss between patients. This guide presents the 80/20 Framework for GLP-1 therapy optimization, positing that medication management accounts for approximately 20% of therapeutic success, while the remaining 80% depends on patient-driven lifestyle modifications, specifically resistance exercise, adequate protein intake, and muscle mass preservation. Drawing on current evidence from systematic reviews and meta-analyses, we demonstrate that lean body mass (LBM) loss during GLP-1 therapy ranges from 25–39% of total weight lost, with profound implications for insulin sensitivity, basal metabolic rate, and long-term outcomes. We present a physiological rationale for exercise-mediated GLUT4 upregulation and glycogen storage optimization as critical adjuncts to GLP-1 therapy, and outline specific clinical pitfalls associated with dose escalation in the absence of adequate lifestyle adherence.
TABLE OF CONTENTS
- 1. Introduction: The Variability Problem in GLP-1 Therapy
- 2. The 80/20 Rule: Redefining the Provider-Patient Paradigm
- 3. The Glucose Tank Model: Why Muscle Mass Is the Key Variable
- 4. Exercise and GLUT4: The Molecular Basis for Improved GLP-1 Outcomes
- 5. Clinical Pitfalls: When Dose Escalation Does More Harm Than Good
- 6. Clinical Recommendations
- 7. Conclusion
- References
- About the Author
- Intellectual Property & Disclosure
1. Introduction: The Variability Problem in GLP-1 Therapy
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have transformed the landscape of obesity and metabolic disease management. Clinical trials have demonstrated remarkable average efficacy: semaglutide producing approximately 15% mean body weight loss over 68 weeks (STEP trials), and tirzepatide achieving up to 22.5% weight reduction over 72 weeks (SURMOUNT-1).¹·² The most recent pipeline candidate, retatrutide, has shown 28.7% weight loss at 68 weeks in Phase 3 trials.³
Yet beneath these impressive averages lies a critical clinical reality: response variability is enormous. Individual weight loss ranges from less than 5% to greater than 20% of body weight, even among patients on identical regimens.⁴ Some patients plateau early despite continued therapy. Others regain weight after discontinuation. A subset maintains metabolic dysfunction despite achieving meaningful weight loss.
This heterogeneity is not random. It reflects the pre-existing metabolic environment within which GLP-1 therapies must operate. GLP-1 RAs address downstream physiology (insulin secretion, appetite suppression, gastric emptying) but do not directly correct the upstream drivers of metabolic disease: chronic inflammation, hormonal dysregulation, adipose tissue dysfunction, and, most critically, the loss of metabolically active lean tissue.⁵
A 2026 systematic review and meta-analysis published in the International Journal of Obesity confirmed that while GLP-1-based treatments drive weight loss primarily through fat reduction, lean body mass (LBM) loss remains a significant concern, with 25–39% of total weight lost coming from fat-free mass across studies.⁶ A 2025 review in Nature Reviews Endocrinology warned that rapid weight loss with GLP-1 RAs can come "at the cost of skeletal muscle, potentially undermining metabolic and functional outcomes."⁷
2. The 80/20 Rule: Redefining the Provider-Patient Paradigm
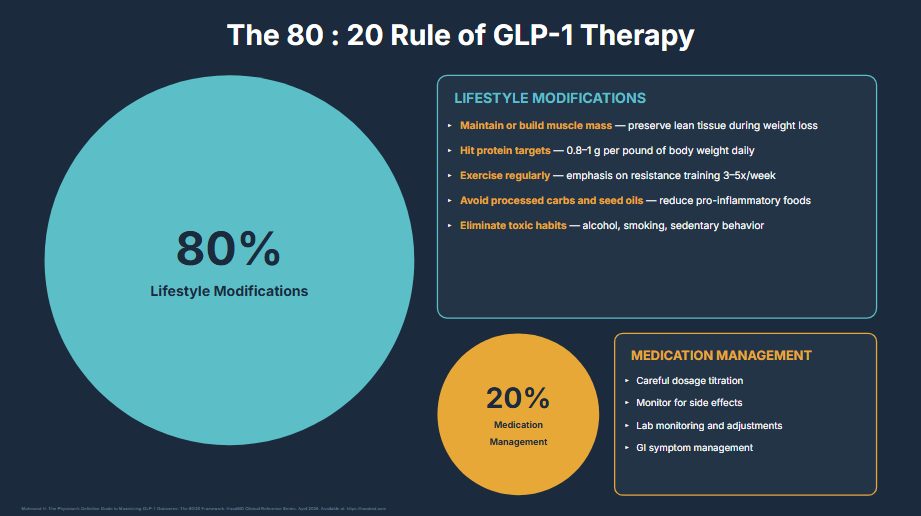
The central thesis of this guide is encapsulated in the 80/20 Rule of GLP-1 Therapy, a clinical framework developed by the author to communicate a fundamental truth to both providers and patients: medication management represents only approximately 20% of the weight loss management equation. The remaining 80% rests on patient-driven lifestyle modifications.
© 2026 Dr. Haad Mahmood, MD. All rights reserved. Original intellectual property. Reproduction prohibited without written permission.
2.1 The 20%: What the Provider Controls
- Careful dosage titration: slow escalation to minimize GI side effects and optimize tolerance
- Side effect monitoring: management of nausea, vomiting, constipation, and rare complications
- Lab monitoring and adjustments: tracking metabolic markers, kidney function, and glycemic control
- GI symptom management: dietary guidance and pharmacologic adjuncts for GI tolerance
These functions are necessary but insufficient. A provider who manages medication flawlessly but fails to educate and hold patients accountable for the 80% will consistently see suboptimal outcomes.
2.2 The 80%: What the Patient Must Own
- Maintain or build muscle mass: preserve lean tissue during caloric deficit
- Hit protein targets: 0.8–1.0 g per pound of body weight daily⁸
- Exercise regularly: emphasis on resistance training 3–5x/week⁹
- Avoid processed carbs and seed oils: reduce pro-inflammatory foods
- Eliminate toxic habits: alcohol, smoking, sedentary behavior
3. The Glucose Tank Model: Why Muscle Mass Is the Key Variable
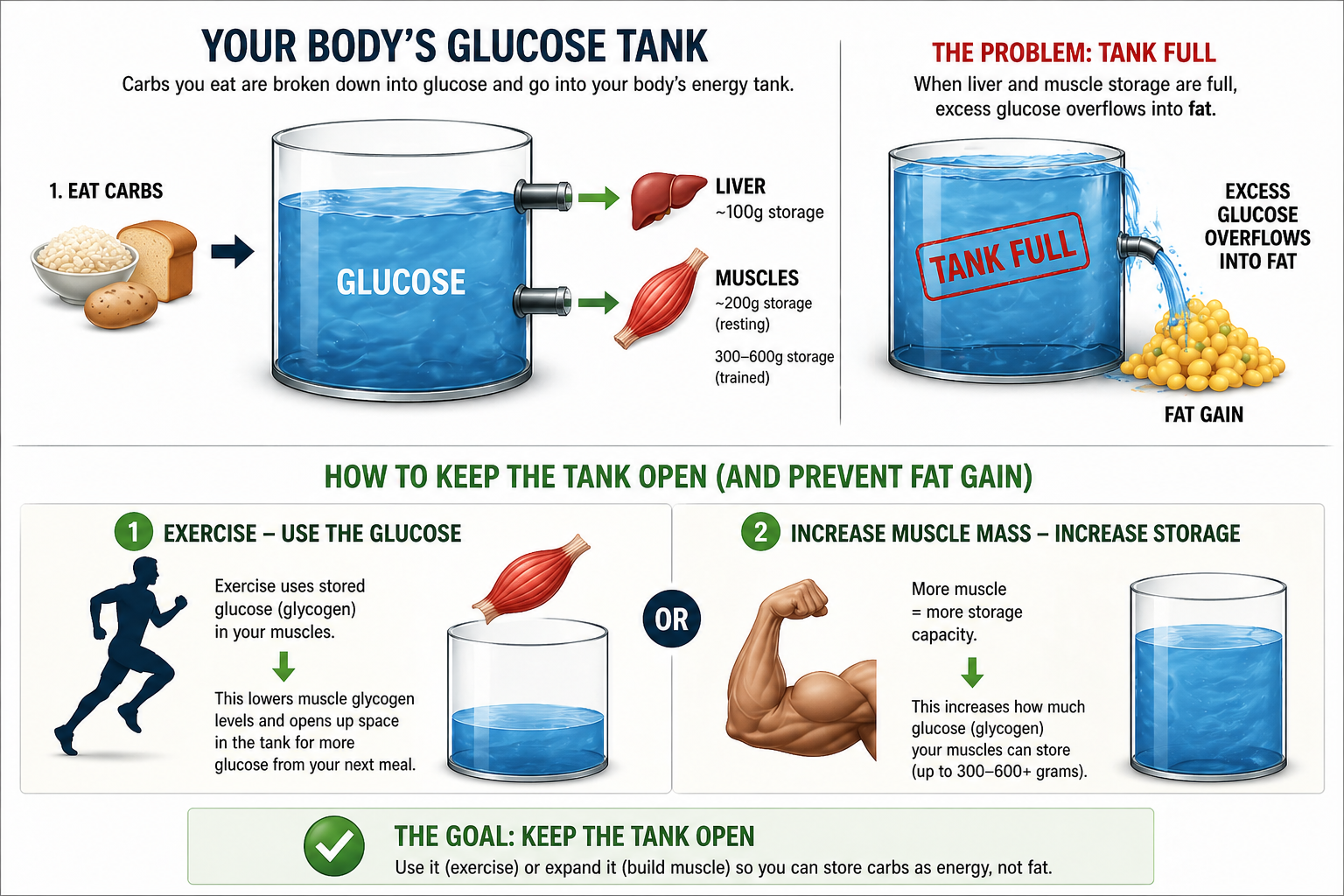
To communicate the physiological rationale for muscle preservation to patients, this guide introduces the Glucose Tank Model, a visual framework for understanding how the body processes, stores, and utilizes glucose, and why muscle mass is the critical variable in preventing fat gain and improving insulin sensitivity.
© 2026 Dr. Haad Mahmood, MD. All rights reserved. Original intellectual property. Reproduction prohibited without written permission.
3.1 The Tank Metaphor
When carbohydrates are consumed, they are broken down into glucose and enter the body’s "energy tank." This tank has two primary storage compartments:
- Liver glycogen storage: approximately 100g capacity
- Muscle glycogen storage: approximately 200–600g capacity (variable, depending on muscle mass)
When both storage compartments are full (the "tank full" state), excess glucose has nowhere to go and is converted to fat through de novo lipogenesis.
3.2 How to Keep the Tank Open
Strategy 1: Exercise. Use the Glucose. Physical activity depletes muscle glycogen stores, opening up space in the tank for glucose from the next meal rather than routing it to fat storage.
Strategy 2: Increase Muscle Mass. Expand the Tank. More muscle means more storage capacity. A patient with greater lean body mass can store 300–600+ grams of glycogen in muscle tissue alone.¹⁰
4. Exercise and GLUT4: The Molecular Basis for Improved GLP-1 Outcomes
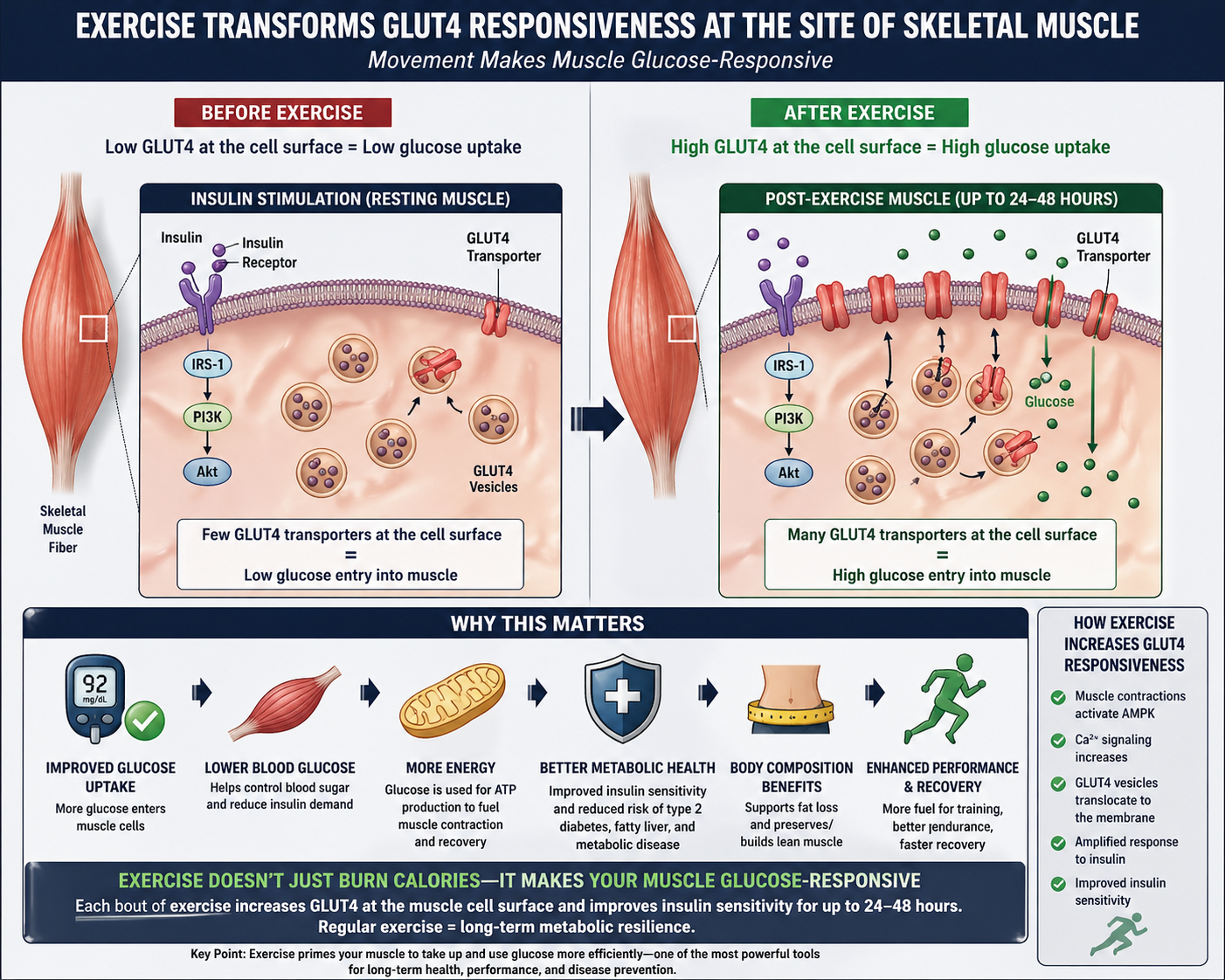
Beyond the macroscopic glucose tank model, there is a compelling molecular mechanism that explains why exercise is not just beneficial but essential during GLP-1 therapy: the upregulation of GLUT4 transporters at the skeletal muscle cell surface.
© 2026 Dr. Haad Mahmood, MD. All rights reserved. Original intellectual property. Reproduction prohibited without written permission.
GLUT4 is the primary insulin-responsive glucose transporter in skeletal muscle. In the resting state, GLUT4 resides in intracellular vesicles. When stimulated by insulin or muscle contraction, GLUT4 translocates to the cell surface, enabling glucose entry. In insulin-resistant individuals, this process is impaired.¹¹·¹²
Each bout of exercise triggers:
- Muscle contraction activates AMPK (AMP-activated protein kinase)
- Ca²⁺ signaling cascades triggered by mechanical contraction
- GLUT4 vesicles translocate to the cell membrane, independent of insulin
- Glucose uptake increases dramatically and remains elevated for 24–48 hours
- Insulin sensitivity improves at the receptor level¹³·¹⁴
Why This Matters for GLP-1 Patients:
- Improved glucose uptake: more glucose enters muscle cells, reducing blood sugar
- Lower blood glucose: helps control A1c and reduces pancreatic beta cell demand
- Better metabolic health: improved insulin sensitivity reduces T2D and metabolic disease risk
- Body composition benefits: promotes fat loss, preserves or builds lean muscle mass
- Enhanced recovery: more fat-burning capacity, better lactate clearance
5. Clinical Pitfalls: When Dose Escalation Does More Harm Than Good
Perhaps the most consequential mistake in GLP-1 management is premature or inappropriate dose escalation. This section identifies specific clinical scenarios where increasing the dose without addressing lifestyle factors produces paradoxically worse outcomes.

© 2026 Dr. Haad Mahmood, MD. All rights reserved. Original intellectual property. Reproduction prohibited without written permission.
5.1 The Dose Escalation Checklist
Dosage should NOT be increased if the patient is not:
- ✘ Exercising at least 3–5 times per week with emphasis on resistance training
- ✘ Meeting protein targets: 0.8–1.0 g per pound of body weight daily
- ✘ Maintaining or building muscle mass (verified through body composition tracking)
- ✘ Losing at an appropriate rate: more than 5–8 lbs per month (avg ~2 lbs/week)
5.2 Consequences of Premature Dose Escalation
DECREASING Muscle Mass. Higher doses suppress appetite further, reducing caloric and protein intake. Without resistance training, the body catabolizes lean tissue. Clinical data shows 34–45% of weight lost can be lean mass.¹⁵
DECREASING Insulin Sensitivity. Less muscle means fewer GLUT4 transporters, reduced glycogen storage, and worsening insulin resistance, even as weight drops on the scale.
DECREASING Basal Metabolic Rate. Lean mass loss can reduce BMR by 100–300+ calories daily, making weight maintenance after discontinuation extremely difficult.¹⁶·¹⁷
6. Clinical Recommendations
- Educate before you prescribe. Before initiating GLP-1 therapy, provide comprehensive education on the 80/20 framework. Patients must understand that medication is a tool, not a solution.
- Mandate body composition tracking. Require baseline and periodic DEXA scans or validated bioimpedance measurements. Track lean body mass separately from total weight.
- Set protein targets at the first visit. Prescribe 0.8–1.0 g of protein per pound of body weight daily. Refer to nutrition counseling if needed. This is non-negotiable.
- Prescribe resistance training as formally as medication. 3–5 sessions per week of progressive resistance training. Document it in the treatment plan. Consider referral to exercise physiologists.
- Gate dose escalation on lifestyle adherence. Do not increase dose unless the patient meets exercise, protein, and body composition benchmarks.
- Monitor beyond the scale. Track fasting insulin, HOMA-IR, inflammatory markers (hs-CRP, cytokines), and hormonal panels alongside weight and body composition.
7. Conclusion
GLP-1 receptor agonists represent a genuine breakthrough in metabolic medicine. Their ability to produce sustained, clinically meaningful weight loss has changed the treatment paradigm for obesity and type 2 diabetes. But they are not magic, and treating them as such is the primary reason for poor outcomes.
The 80/20 Framework presented in this guide is both a clinical philosophy and a practical tool. It reframes the provider-patient relationship: the physician’s role is to manage the 20% (medication) with precision, while educating and empowering the patient to own the 80% (lifestyle). The glucose tank model provides an intuitive, patient-friendly framework for understanding why muscle mass matters. The GLUT4 mechanism provides the molecular evidence. And the clinical pitfalls section provides the guardrails against the most common management errors.
The evidence is clear: the quality of GLP-1 weight loss is determined not by the dose, but by the metabolic environment in which the drug operates. Building and preserving that environment through resistance training, adequate protein, and disciplined lifestyle modification is the single greatest determinant of whether a patient achieves lasting metabolic transformation or simply loses weight on a scale while their metabolic health quietly deteriorates.
Prescribe the lifestyle.”
— Dr. Haad Mahmood, MD
“Don’t increase the dose unless you can increase the activity.”
— Dr. Haad Mahmood, MD
References
- Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989-1002. (STEP 1 Trial)
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387(3):205-216. (SURMOUNT-1)
- Eli Lilly and Company. TRIUMPH-4: Retatrutide Phase 3 results. Press release, December 2025. 28.7% weight loss at 68 weeks.
- Mahmood H. Variability in GLP-1 Clinical Outcomes [Presentation slide]. Correlating GLP-1 Outcomes with Advanced Lab Panels. 2026. Original intellectual property of Dr. Haad Mahmood, MD.
- Mahmood H. GLP-1 Mechanism vs. Disease Complexity [Presentation slide]. Correlating GLP-1 Outcomes with Advanced Lab Panels. 2026. Original IP of Dr. Haad Mahmood, MD.
- Sawicka-Gutaj N, Gruszczyński D, et al. GLP-1 agonists and changes in body mass and composition in adults with overweight or obesity. Int J Obes. 2026. doi:10.1038/s41366-026-02088-1
- Sanchis-Gomar F, Neeland IJ, Lavie CJ. Balancing weight and muscle loss in GLP1 receptor agonist therapy. Nat Rev Endocrinol. 2025;21:584-585.
- ACLM, ASN, OMA, TOS. Nutritional priorities to support GLP-1 therapy for obesity: a joint Advisory. Am J Clin Nutr. 2025.
- University of Exeter. Function and Lean Mass Preservation With Resistance Exercise During a GLP1RA Treatment (FLEX). ClinicalTrials.gov: NCT07457437. 2025.
- Tinsley GM, Heymsfield SB. Fundamental body composition principles provide context for fat-free and skeletal muscle loss with GLP-1 RA treatments. J Endocr Soc. 2024;8(11):bvae164.
- Jeon JY, Choi SE, Ha ES, et al. GLP-1 improves palmitate-induced insulin resistance in human skeletal muscle via SIRT1 activity. Int J Mol Med. 2019;44(3):1161-1171.
- Tian X, Gao Y, Kong M, et al. GLP-1 receptor agonist protects palmitate-induced insulin resistance in skeletal muscle cells by up-regulating sestrin2. Sci Rep. 2023;13:9446.
- Codella R, Senesi P, Luzi L. GLP-1 agonists and exercise: the future of lifestyle prioritization. Front Clin Diabetes Healthc. 2025;6.
- Chai W, Dong Z, Wang N, et al. Glucagon-like peptide 1 recruits microvasculature and increases glucose use in muscle via a nitric oxide-dependent mechanism. Diabetes. 2012;61(4):888-896.
- ClearMetabolic. GLP-1 Body Composition Guide: Protect Muscle While Losing Fat. Updated March 2026. Clinical trial data: 34-45% lean mass loss ratios.
- Rossi G, Bucciarelli L, Mananguite CL, et al. Muscle loss and GLP-1R agonists use. Acta Diabetol. 2025;63(2):333-342.
- Mills T. The GLP-1 aftermath: what the science says about muscle loss and cellular aging. Harvard Science Review. February 23, 2026.
- Mahmood H. The 80:20 Rule of GLP-1 Therapy [Figure 1]. Correlating GLP-1 Outcomes with Advanced Lab Panels: Cytokines, Metabolic Markers, and Hormones. 2026. Original IP of Dr. Haad Mahmood, MD.
- Mahmood H. Your Body’s Glucose Tank [Figure 2]. Correlating GLP-1 Outcomes with Advanced Lab Panels: Cytokines, Metabolic Markers, and Hormones. 2026. Original IP of Dr. Haad Mahmood, MD.
- Mahmood H. Exercise Transforms GLUT4 Responsiveness at the Site of Skeletal Muscle [Figure 3]. Correlating GLP-1 Outcomes with Advanced Lab Panels: Cytokines, Metabolic Markers, and Hormones. 2026. Original IP of Dr. Haad Mahmood, MD.
- Mahmood H. Major GLP-1 Mismanagement Pitfalls [Figure 4]. Correlating GLP-1 Outcomes with Advanced Lab Panels: Cytokines, Metabolic Markers, and Hormones. 2026. Original IP of Dr. Haad Mahmood, MD.
Suggested Citation: Mahmood H. The Physician’s Definitive Guide to Maximizing GLP-1 Outcomes: The 80/20 Framework. HaadMD Clinical Reference Series. April 2026. Available at: https://haadmd.com