
The Physician's Guide to Cortisol Dysfunction in Metabolic Disease
ABSTRACT
Cortisol, the body's primary glucocorticoid, plays a central role in metabolic regulation, immune modulation, and energy homeostasis. However, chronic hypothalamic-pituitary-adrenal (HPA) axis dysregulation leads to a progressive deterioration of adrenal function, from cortisol overdrive to eventual burnout, with profound implications for metabolic health, thyroid function, and treatment outcomes. This guide presents a clinical framework for understanding cortisol dysfunction across three distinct phases, examines the mechanistic relationship between chronic stress, reverse T3 (rT3) accumulation, and thyroid pathway interference, and outlines evidence-based treatment strategies for cortisol management. We demonstrate that DHEA-S serves as a clinically useful biomarker for evaluating long-term HPA axis burden and adrenal reserve, and that unaddressed cortisol dysfunction represents a significant and underappreciated barrier to achieving durable metabolic outcomes.
TABLE OF CONTENTS
- 1. Introduction: Cortisol and the Metabolic Landscape
- 2. The HPA Axis: Hypothalamic-Pituitary-Adrenal Regulation
- 3. The Three Phases of Cortisol Burnout
- 4. DHEA-S and SHBG: Hormonal Context of Metabolic Function
- 5. Thyroid Hormone Pathway: How Reverse T3 (rT3) Blocks T3
- 6. Cortisol, Reward Signaling, and Appetite Override
- 7. Clinical Management: Treatment of Elevated Cortisol and Stress
- 8. Clinical Recommendations
- 9. Conclusion
- References
- About the Author
- Intellectual Property and Disclosure
1. Introduction: Cortisol and the Metabolic Landscape
The hormonal environment profoundly shapes metabolic rate, body composition, appetite regulation, and insulin sensitivity , all of which determine the effectiveness of metabolic interventions. Among the hormonal axes that influence metabolic outcomes, the hypothalamicpituitary-adrenal (HPA) axis and its primary effector hormone, cortisol, occupy a uniquely central position.
Cortisol is essential for survival. It mobilizes glucose during acute stress, modulates immune responses, and regulates circadian energy availability. However, when the stress response becomes chronic (driven by psychosocial stress, sleep disruption, caloric restriction, environmental toxins, or metabolic disease itself) the HPA axis shifts from adaptive regulation to maladaptive dysfunction.
This dysfunction does not occur in isolation. Chronic cortisol dysregulation impairs insulin signaling, promotes visceral adiposity, disrupts thyroid hormone conversion, and directly antagonizes appetite-suppressive mechanisms. Patients with unrecognized HPA axis dysfunction frequently present with treatment resistance, early plateau, or paradoxical weight regain despite adequate pharmacologic intervention.
This guide provides a systems-level framework for understanding cortisol dysfunction in the context of metabolic disease. We present a three-phase model of cortisol burnout, examine the thyroid-cortisol axis, and outline clinical strategies for diagnosis and management.
2. The HPA Axis: Hypothalamic-Pituitary-Adrenal Regulation
The HPA axis represents the body's central stress response system, coordinating the release of cortisol through a cascading signaling pathway:
- The hypothalamus detects stress signals and releases corticotropin-releasing hormone (CRH)
- CRH stimulates the anterior pituitary to secrete adrenocorticotropic hormone (ACTH)
- ACTH acts on the adrenal cortex to stimulate cortisol synthesis and release
- Cortisol exerts negative feedback on both the hypothalamus and pituitary, completing the regulatory loop
Under normal conditions, this system maintains tight homeostatic control, with cortisol following a predictable diurnal pattern: peak levels in the early morning (the cortisol awakening response) and a gradual decline through the evening, reaching its nadir around midnight.
2.1 Steroidogenesis and Cortisol's Place in the Hormonal Cascade
Cortisol is synthesized from cholesterol through the steroidogenesis pathway. This pathway is shared with other critical hormones, including DHEA, testosterone, estradiol, and aldosterone. Under chronic stress, the adrenal glands preferentially shunt precursors toward cortisol production (a phenomenon sometimes referred to as the "pregnenolone steal") at the expense of sex hormone and DHEA synthesis.
This has direct clinical implications: chronically elevated cortisol demand depletes DHEA-S reserves and may contribute to low testosterone, estradiol deficiency, and reduced SHBG levels , all of which independently impair metabolic function.
2.2 When the HPA Axis Becomes Maladaptive
The HPA axis evolved for acute, time-limited stress responses. Modern chronic stressors (psychological stress, sleep deprivation, ultra-processed diets, environmental toxin exposure, and sedentary behavior) create sustained activation that the system was not designed to handle. Over time, this leads to the progressive dysfunction described in Section 3.
3. The Three Phases of Cortisol Burnout
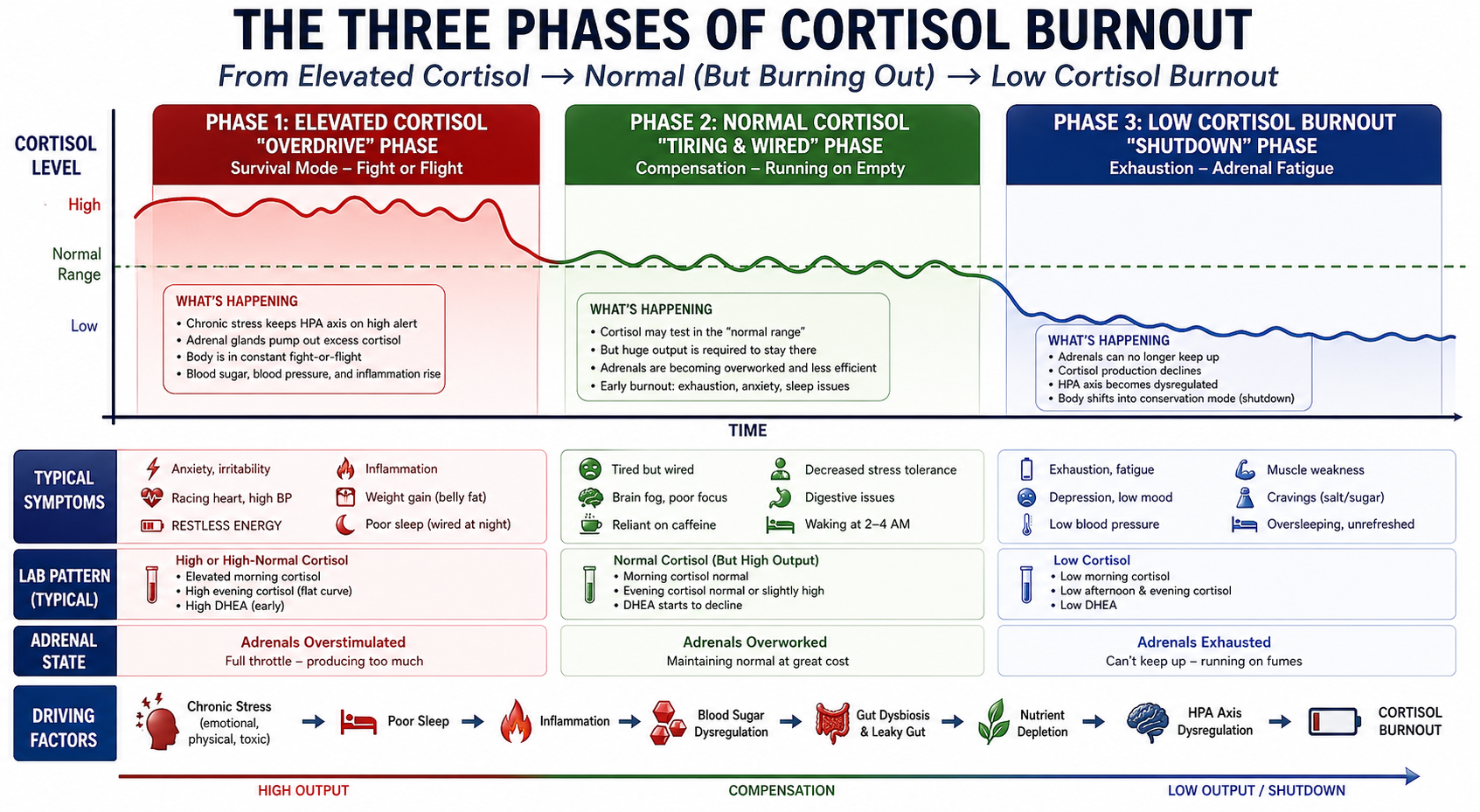
The progression from healthy HPA axis function to cortisol burnout follows a predictable clinical trajectory that can be mapped across three distinct phases. Understanding these phases allows clinicians to identify where a patient falls on the dysfunction spectrum and tailor interventions accordingly.
© 2026 Dr. Haad Mahmood, MD. All rights reserved. Original intellectual property. Reproduction prohibited without written permission.
Mahmood H. The Three Phases of Cortisol Burnout: Utilizing DHEA-S as a Useful Biomarker to Evaluate Stress Markers. HaadMD. 2026. https://haadmd.com
3.1 Phase 1: Elevated Cortisol: "Overdrive"
In the initial phase, the adrenal glands respond to chronic stress with sustained cortisol overproduction. This is the body's attempt to maintain homeostasis under persistent threat signals. Patients in this phase often present with:
- Anxiety and irritability with racing thoughts
- Insomnia or disrupted sleep architecture
- Central adiposity and weight gain, particularly visceral fat accumulation
- Elevated blood pressure and heart rate
- Sugar and carbohydrate cravings driven by cortisol-mediated glucose mobilization
- Elevated fasting insulin as cortisol drives hepatic gluconeogenesis and peripheral insulin resistance
Laboratory findings typically show elevated morning cortisol, initially elevated or normal DHEAS, rising inflammatory markers (hs-CRP, IL-6), and early insulin resistance patterns.
3.2 Phase 2: Normal Cortisol: "Tiring and Wired"
As chronic stress persists, the adrenal glands begin to lose their capacity for sustained overproduction. Cortisol levels may normalize on standard testing, but this apparent normality is deceptive ; it represents compensation, not resolution. The system is working harder to produce less.
- Fatigue becomes prominent despite seemingly normal cortisol values
- The "wired but tired" phenomenon: sympathetic nervous system activation persists even as cortisol output declines
- Exercise recovery deteriorates significantly
- Brain fog and cognitive difficulty emerge
- Caffeine dependence increases as patients seek pharmacologic stimulation to compensate for declining endogenous drive
The critical lab finding in Phase 2 is declining DHEA-S. While cortisol may appear normal, the falling DHEA-S reveals that adrenal reserve is being consumed. Reverse T3 (rT3) begins to rise as the body shifts from active thyroid hormone metabolism to a conservation state.
3.3 Phase 3: Low Cortisol: "Shutdown"
Phase 3 represents the end-stage of chronic HPA axis dysregulation. The adrenal glands can no longer maintain adequate cortisol output, and patients experience systemic consequences of cortisol insufficiency:
- Profound, debilitating fatigue that is not relieved by rest
- Complete inability to handle additional stressors (emotional or physical)
- Orthostatic hypotension and salt cravings (reflecting aldosterone pathway disruption)
- Immune dysfunction with frequent illness
- Depression, apathy, and emotional flatness
- Complete burnout ; patients describe feeling like "a shell of themselves"
Laboratory findings show low cortisol (both AM and PM), severely depleted DHEA-S, low free T3 with elevated rT3, and low SHBG. These patients have lost their metabolic resilience entirely.
4. DHEA-S and SHBG: Hormonal Context of Metabolic Function
Two biomarkers provide critical context for evaluating the hormonal-metabolic phenotype in patients with cortisol dysfunction: DHEA-S and SHBG.
4.1 DHEA-S: Adrenal Reserve Marker
DHEA-S (dehydroepiandrosterone sulfate) is a marker of adrenal reserve and long-term HPA axis output. It supports metabolic resilience and anti-inflammatory balance. Key clinical considerations:
- DHEA-S reflects cumulative adrenal burden over weeks to months, making it more stable than cortisol for longitudinal tracking
- Low levels are associated with chronic stress and reduced adaptive capacity during weight loss
- Depleted DHEA-S indicates an adrenal system under sustained burden that limits the body's ability to respond to metabolic interventions
- DHEA-S declines progressively across the three phases of cortisol burnout, making it a useful staging biomarker
4.2 SHBG: Metabolic Syndrome Indicator
SHBG (sex hormone-binding globulin) directly affects the bioavailability of testosterone and estradiol, both of which influence metabolic rate, body composition, and insulin sensitivity.
- Low SHBG indicates hyperinsulinemia and metabolic syndrome
- Low SHBG combined with high insulin reflects persistent insulin resistance that reduces the effectiveness of metabolic therapies
- SHBG levels help differentiate whether a patient's treatment resistance is primarily hormonal versus purely metabolic
Clinical Implication: DHEA-S and SHBG together help identify the hormonal-metabolic phenotype impacting response to therapy , particularly in patients who appear to be on adequate treatment but show blunted or plateauing response. A patient with low DHEA-S and low SHBG is operating with both depleted adrenal reserve and active insulin resistance . This combination profoundly limits therapeutic effectiveness.
5. Thyroid Hormone Pathway: How Reverse T3 (rT3) Blocks T3
Chronic cortisol dysregulation has a direct and clinically significant impact on thyroid hormone metabolism. Understanding this pathway is essential for managing metabolic patients, as thyroid function determines basal metabolic rate, energy expenditure, and body composition.
© 2026 Dr. Haad Mahmood, MD. All rights reserved. Original intellectual property. Reproduction prohibited without written permission.
Mahmood H. Thyroid Hormone Pathway and How Reverse T3 (rT3) Blocks T3. HaadMD. 2026. https://haadmd.com
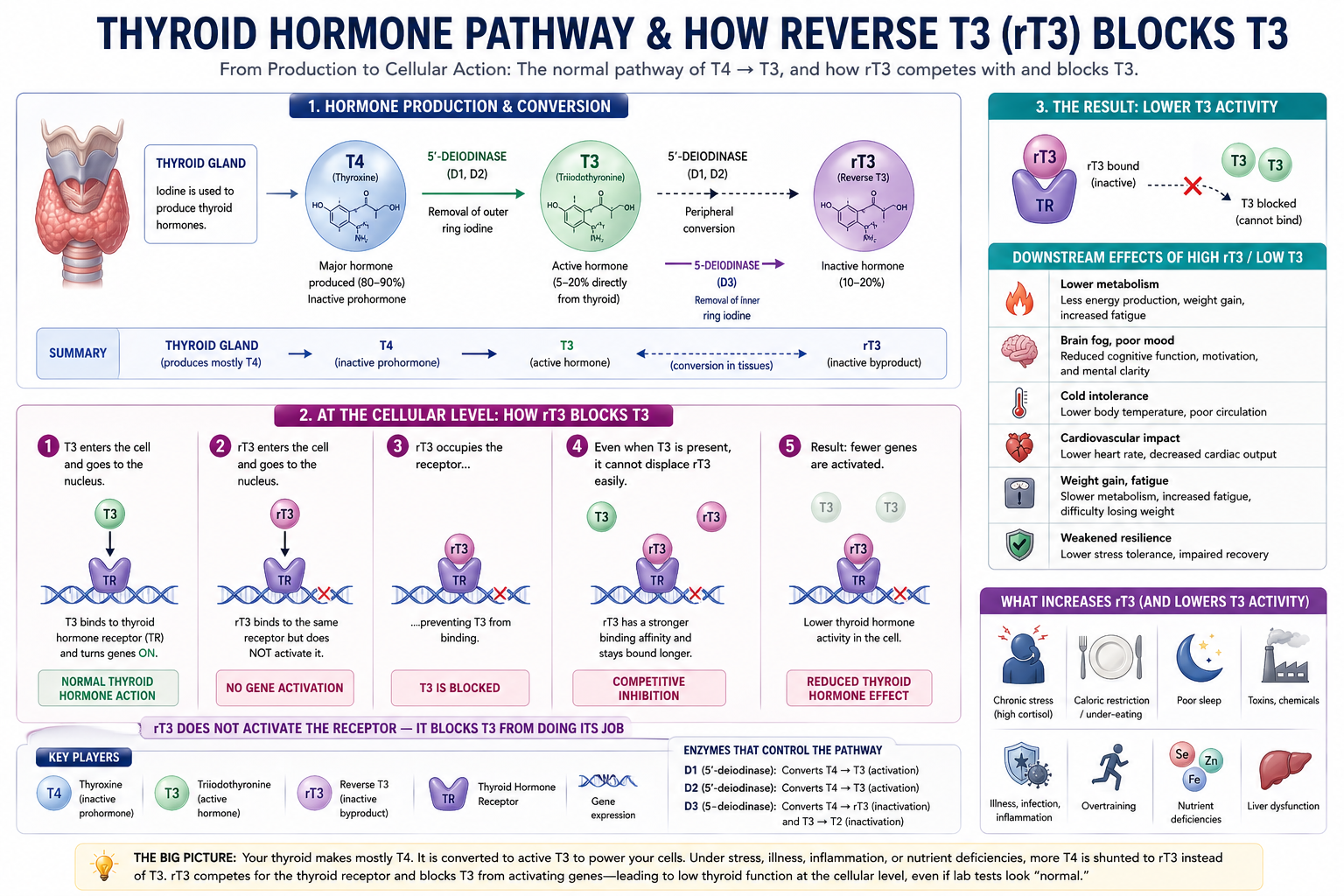
5.1 The T4-to-T3 Conversion Problem
The thyroid gland produces primarily T4 (thyroxine), which serves as an inactive precursor. T4 must be converted to T3 (triiodothyronine) (the metabolically active thyroid hormone) by deiodinase enzymes in peripheral tissues. However, T4 can also be converted to reverse T3 (rT3), an inactive metabolite that competes with T3 at the thyroid hormone receptor.
Under conditions of chronic stress, the body preferentially converts T4 to rT3 rather than T3. This is an evolutionary conservation mechanism ; the body reduces metabolic rate to preserve energy during perceived threat. In modern chronic stress, this mechanism becomes maladaptive: patients develop functional hypothyroidism with normal TSH and total T4 levels but inadequate active T3 at the cellular level.
5.2 Clinical Consequences of Elevated rT3
- Decreased basal metabolic rate , directly reducing energy expenditure and impeding weight loss
- Fatigue and cold intolerance despite normal standard thyroid panels
- Weight gain and profound difficulty losing weight, even with caloric restriction and pharmacologic intervention
- Impaired lipid metabolism and increased cardiovascular risk
- Reduced effectiveness of metabolic therapies . The metabolic rate reduction directly opposes the energy balance changes that treatment is designed to produce
5.3 What Increases rT3
The primary drivers of increased rT3 production are:
- Chronic stress . Elevated cortisol directly promotes deiodinase Type 3 activity, shunting T4 toward rT3
- Calorie restriction . Aggressive caloric deficits signal energy conservation, increasing rT3
- Poor sleep quality and duration . Disrupted circadian rhythm alters thyroid hormone metabolism
- Environmental toxins and chemicals . Endocrine disruptors interfere with deiodinase enzyme function
- Systemic inflammation . Pro-inflammatory cytokines (IL-6, TNF-alpha) promote rT3 production
6. Cortisol, Reward Signaling, and Appetite Override
Cortisol influences appetite through two distinct but interconnected central nervous system pathways: hypothalamic-pituitary signaling and dopaminergic reward circuits. This dual mechanism creates a powerful appetite drive that can override satiety signaling from pharmacologic and endogenous sources.
6.1 Central Appetite Pathways Affected
Elevated cortisol produces the following appetite-related effects:
- Increased cravings for energy-dense, high-glycemic foods . Cortisol preferentially drives desire for simple carbohydrates and high-fat foods that rapidly elevate blood glucose
- Stress-driven eating independent of caloric need . The HPA axis activation creates a compulsive eating pattern unrelated to actual energy requirements
- Increased hedonic ("reward-based") food intake . Cortisol amplifies dopaminergic reward signaling, making food consumption a stress-coping mechanism
- Disrupted leptin signaling and impaired satiety perception . Elevated cortisol blunts the brain's ability to recognize satiety signals from leptin and other gut hormones
6.2 Appetite Suppression Interference
Appetite-suppressive therapies work primarily via brainstem and hypothalamic pathways , the same pathways that cortisol disrupts. Elevated cortisol effectively competes with pharmacologic appetite suppression at the central level, creating a competition:
- Appetite therapy signals: "You are full, stop eating"
- Cortisol signals: "You are threatened, eat more energy-dense food now"
- Dopamine reward circuits, amplified by cortisol, reinforce eating as a stress-coping behavior
Patients with high cortisol experience less appetite suppression and have a higher likelihood of plateau or rebound. Many patients and providers attribute this to treatment resistance or dose inadequacy, when the actual problem is unaddressed HPA axis dysregulation.
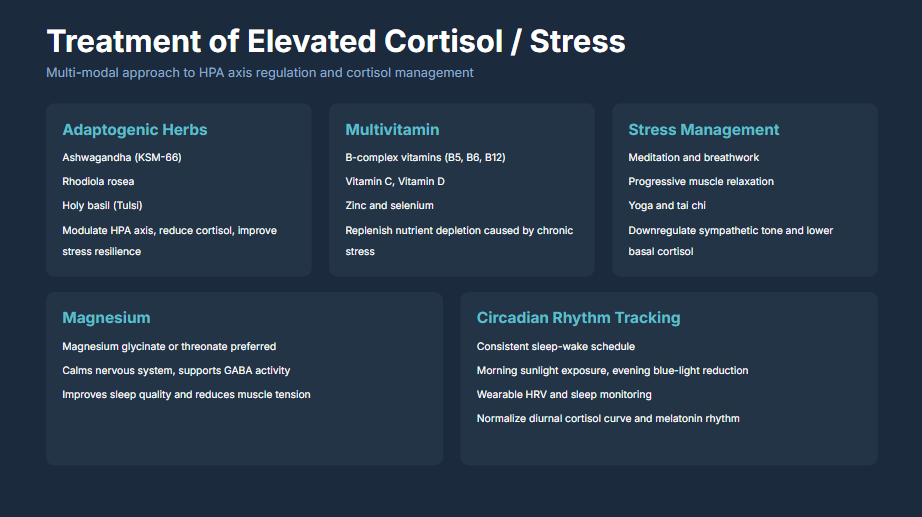
7. Clinical Management: Treatment of Elevated Cortisol and Stress
Management of cortisol dysfunction requires a multi-modal approach targeting HPA axis regulation through five complementary therapeutic domains.
© 2026 Dr. Haad Mahmood, MD. All rights reserved. Original intellectual property. Reproduction prohibited without written permission.
7.1 Adaptogenic Herbs
Adaptogens are botanical agents that modulate the stress response by normalizing HPA axis function. Key agents include:
- Ashwagandha (KSM-66 extract): The most studied adaptogen for cortisol reduction. Randomized controlled trials demonstrate significant reductions in serum cortisol and perceived stress. KSM-66 is the standardized root extract with the strongest evidence base.
- Rhodiola rosea: Acts on serotonergic and dopaminergic pathways to improve stress resilience, reduce fatigue, and support cognitive function under stress.
- Holy basil (Tulsi): Modulates cortisol and supports adrenal function while providing anti-inflammatory and antioxidant activity.
7.2 Targeted Nutritional Support
Chronic stress depletes specific micronutrients essential for HPA axis function and cortisol metabolism:
- B-complex vitamins (B5, B6, B12): B5 (pantothenic acid) is critical for adrenal cortex function and cortisol synthesis. B6 supports neurotransmitter production. B12 supports methylation and nervous system function.
- Vitamin C: The adrenal glands contain the highest concentration of vitamin C in the body. Chronic stress depletes adrenal vitamin C reserves.
- Vitamin D: Supports immune modulation and has direct effects on HPA axis regulation.
- Zinc and selenium: Essential cofactors for thyroid hormone conversion (relevant to the rT3 pathway) and immune function.
7.3 Stress Management Techniques
Non-pharmacologic interventions that directly downregulate sympathetic nervous system tone:
- Meditation and breathwork: Diaphragmatic breathing and mindfulness meditation have demonstrated reductions in salivary cortisol in controlled studies.
- Progressive muscle relaxation: Systematic tension-release protocols that reduce somatic stress holding patterns.
- Yoga and tai chi: Combine physical movement, breathwork, and mindfulness for comprehensive parasympathetic activation.
7.4 Magnesium Supplementation
Magnesium plays a critical role in HPA axis regulation:
- Magnesium glycinate or threonate are preferred forms . Glycinate is preferred for sleep and muscle relaxation; threonate for cognitive support and blood-brain barrier penetration
- Supports GABA receptor activity, promoting parasympathetic tone
- Improves sleep quality and reduces nocturnal cortisol
- Reduces muscle tension and supports recovery from exercise
7.5 Circadian Rhythm Optimization
Restoring the normal diurnal cortisol pattern is essential for long-term HPA axis recovery:
- Consistent sleep-wake schedule: Same bedtime and wake time daily, including weekends
- Morning sunlight exposure: 10-20 minutes of natural light within 30 minutes of waking to anchor the cortisol awakening response
- Evening blue-light reduction: Minimize screen exposure 1-2 hours before sleep to support melatonin production
- Wearable HRV and sleep monitoring: Heart rate variability tracking provides objective data on autonomic nervous system balance and recovery status
8. Clinical Recommendations
- Screen for HPA axis dysfunction in all metabolic patients. Before initiating or escalating metabolic therapy, evaluate cortisol status. Order morning cortisol, DHEA-S, free T3, reverse T3, and SHBG as part of the baseline hormonal assessment.
- Stage the patient using the Three Phases framework. Identify whether the patient is in Phase 1 (overdrive), Phase 2 (compensation), or Phase 3 (burnout). Treatment strategy differs significantly by phase.
- Address cortisol dysfunction before escalating pharmacologic dose. Patients with active HPA axis dysregulation will show blunted treatment response. Cortisol management should be initiated concurrently or prior to dose increases.
- Monitor DHEA-S longitudinally. DHEA-S provides a more stable indicator of adrenal reserve than single-point cortisol measurements. Track it at baseline and every 3-6 months.
- Check the rT3:T3 ratio in patients with fatigue and weight loss resistance. A high ratio indicates stress-mediated thyroid suppression that standard TSH/T4 panels will miss entirely.
- Implement multi-modal cortisol management. Combine adaptogenic herbs, targeted nutritional support, stress management techniques, magnesium supplementation, and circadian rhythm optimization. No single intervention addresses the full spectrum of HPA axis dysfunction.
- Integrate cortisol management into the treatment framework. Cortisol management falls squarely within the patient-driven lifestyle modifications that determine therapeutic success. Educate patients on the direct connection between stress management and treatment outcomes.
9. Conclusion
Cortisol dysfunction represents one of the most clinically significant and underappreciated barriers to achieving durable metabolic outcomes. The three-phase model of cortisol burnout provides clinicians with a practical framework for staging patients, selecting interventions, and predicting treatment response.
The mechanistic connections are clear: chronic cortisol elevation drives insulin resistance, promotes visceral adiposity, suppresses thyroid hormone activity through rT3 accumulation, and directly antagonizes appetite suppression through reward pathway amplification. Patients with unaddressed HPA axis dysfunction operate with a fundamentally compromised metabolic environment . This limits the effectiveness of even the most potent pharmacologic interventions.
The integration of cortisol assessment and management into metabolic care is not optional ; it is essential. DHEA-S provides a clinically accessible window into adrenal reserve. Reverse T3 reveals hidden thyroid dysfunction. And the multi-modal treatment approach outlined in this guide offers a practical, evidence-informed framework for restoring HPA axis function.
The message to clinicians is clear: metabolic therapies operate within a hormonal environment that you and your patient must build together. Cortisol management is not a supplement to metabolic care ; it is a foundation of it.
Address the cortisol, and the medication works."
~ Dr. Haad Mahmood, MD
References
- Mahmood H. The Three Phases of Cortisol Burnout: Utilizing DHEA-S as a Useful Biomarker to Evaluate Stress Markers [Figure 1]. Correlating Outcomes with Advanced Lab Panels: Cytokines, Metabolic Markers, and Hormones. 2026. Original intellectual property of Dr. Haad Mahmood, MD.
- Mahmood H. Thyroid Hormone Pathway and How Reverse T3 (rT3) Blocks T3 [Figure 2]. Correlating Outcomes with Advanced Lab Panels: Cytokines, Metabolic Markers, and Hormones. 2026. Original IP of Dr. Haad Mahmood, MD.
- Mahmood H. Treatment of Elevated Cortisol and Stress [Figure 3]. Correlating Outcomes with Advanced Lab Panels. 2026. Original IP of Dr. Haad Mahmood, MD.
- Mahmood H. The Physician's Definitive Guide to Maximizing Metabolic Outcomes. HaadMD Clinical Reference Series. April 2026. Available at: https://haadmd.com
- Häggström M, Richfield D. Diagram of the pathways of human steroidogenesis. WikiJournal of Medicine. 2014;1(1). CC BY-SA 3.0, via Wikimedia Commons.
- LaValle Metabolic Institute. Metabolic Activation Pathways. Used with attribution.
- Charmandari E, Tsigos C, Chrousos G. Endocrinology of the stress response. Annu Rev Physiol. 2005;67:259-284.
- Chandrasekhar K, Kapoor J, Anishetty S. A prospective, randomized double-blind, placebo-controlled study of safety and efficacy of a high-concentration full-spectrum extract of ashwagandha root in reducing stress and anxiety in adults. Indian J Psychol Med. 2012;34(3):255-262.
- Panossian A, Wikman G. Effects of adaptogens on the central nervous system and the molecular mechanisms associated with their stress-protective activity. Pharmaceuticals (Basel). 2010;3(1):188-224.
- Boyle NB, Lawton C, Dye L. The effects of magnesium supplementation on subjective anxiety and stress: a systematic review. Nutrients. 2017;9(5):429.
- Nicolaides NC, Charmandari E, Kino T, Chrousos GP. Stress-related and circadian secretion and target tissue actions of glucocorticoids: impact on health. Front Endocrinol (Lausanne). 2017;8:70.
- de Herder WW, et al. Adrenal insufficiency. Lancet. 2003;361(9372):1881-1893.
- Bianco AC, et al. Biochemistry, cellular and molecular biology, and physiological roles of the iodothyronine selenodeiodinases. Endocr Rev. 2002;23(1):38-89.
- Peeters RP, et al. Reduced activation and increased inactivation of thyroid hormone in tissues of critically ill patients. J Clin Endocrinol Metab. 2003;88(7):3202-3211.
- Epel E, Lapidus R, McEwen B, Brownell K. Stress may add bite to appetite in women: a laboratory study of stressinduced cortisol and eating behavior. Psychoneuroendocrinology. 2001;26(1):37-49.
- Dallman MF, et al. Chronic stress and body composition: stress-induced hyperphagia and comfort food. Proc Natl Acad Sci USA. 2003;100(20):11696-11701.